|
|
|
|
When Randomisation is not Enough: Masking for Efficacy
Trials of Skin Disease, Ulcers and Wound Infections
In a previous News Blog [1] we discussed endpoint measurement for trials of wound infection, where the observers were not ‘blinded’ (not masked to the intervention group). Such an approach is simply not adequate, even if the observers use ‘strict criteria’.[1] This is because of subjectivity in the interpretation of the criteria and, more especially, because of reactivity. Reactivity means that observers are influenced, albeit sub-consciously, by knowledge of the group to which patients have been assigned (treatment or not). Such reactivity is an important source of bias in science.[2]
We are proposing a trial of a promising treatment for recurrent leprosy ulcers that we would like to carry out in the Leprosy Mission Hospital in Kathmandu, Nepal. We plan to conduct an efficacy trial of a regenerative medicine (RM) technique where a paste is made from the buffy coat layer of the patient’s own blood. This is applied to the ulcer surface at the time of dressing change. The only difference in treatment will be whether or not the RM technique is applied when the regular change of wet dressing is scheduled. We will measure, amongst other things, the rate of healing on the ulcers and time to complete healing and discharge from hospital.
Patients will be randomised so as to avoid selection bias and, as the primary endpoints in this efficacy trial are measured during the hospital sojourn (and patients seldom discharge themselves), we are mainly concerned with outcome bias as far as endpoints regarding ulcer size are concerned.
One obvious way to get around the problem of reactivity is to use a well described method in which truly masked observers, typically based off-site, measure ulcer size using photographs. Measurements are based on a sterile metal ruler positioned at the level of the ulcer to standardise the measurement irrespective of the distance of the camera. The measurement can be done manually or automated by computer (or both). But is that enough? It has been argued that bias can still arise, not at the stage where photographs are analysed, but rather at the earlier stage of photograph acquisition. This argument holds that, again perhaps sub-consciously, those responsible for taking the photograph can affect its appearance. The question of blinding / masking of medical images is a long-standing topic of debate.
The ‘gold standard’ method is to have an independent observer arrive on the scene at the appropriate time to make the observations (and take any photographs). Such a method would be expensive (and logistically challenging over long distances). So, an alternative would be to deploy such an observer for a random sub-set of cases. This method may work but it has certain disadvantages. First, it would be tricky to choreograph as it would disrupt the work flow in settings such as that described above. Second, to act as a method of audit, it would need to be used alongside the existing method (making the method still more ‘unwieldy’). Third, the method of preparing the wound would still lie in the hands of the clinical team, and arguably still be subject to some sort of subconscious ‘manipulation’ (unless the observer also provided the clinical care). Fourth, given that agreement would not be exact between observers, a threshold would have to be agreed regarding the magnitude of difference between the standard method and the monitoring method that would be regarded as problematic. Fifth, it would not be clear how to proceed if such a threshold was crossed. While none of these problems are necessarily insurmountable, they are sufficiently problematic to invite consideration of further methods. What might augment or replace standard third party analysis of photographic material?
Here we draw our inspiration from a trial of surgical technique in the field of ophthalmology/orbital surgery.[3] In this trial, surgical operations were video-taped in both the intervention and control groups. With permission of patients, we are considering such an approach in our proposed trial. The vast majority of ulcers are on the lower extremities, so patients’ faces would not appear in the videos. The videos could be arranged so that staff were not individually identifiable, though they could be redacted if and where necessary. We would like to try to develop a method whereby the photographs were directed in real time by remote video link, but pending the establishment of such a link, we propose that each procedure (dressing change) is video-taped, adhering to certain guidelines (for example, shot in high-definition, moving the camera to give a full view of the limb from all sides, adequate lighting, a measurement instrument is included in the shot, etc.). We propose that measurements are made both in the usual way (from mobile phone photographs), and from ‘stills’ obtained from the video-tapes. Each could be scored by two independent, off-site observers. Furthermore the videos could be used as a method of ‘ethnographic’ analysis of the process to surface any material differences between patients in each trial arm in lighting, preparation of ulcer sites, time spent on various stages of the procedure and photograph acquisition, and so on.
Would this solve the problem? After all, local clinicians would still prepare the ulcer site for re-bandaging and, insofar as they may be able to subconsciously manipulate the situation, this risk has not been vitiated. However, we hypothesise that the video will work a little like a black box on an aeroplane; it cannot stop things happening, but it provides a powerful method to unravel what did happen. The problem we believe we face is not deliberate maleficence, but subtle bias at the most. We think that by using the photographic approach, in accordance with guidelines for such an approach,[4] we already mitigate the risk of outcome measurement bias. We think that by introducing a further level of scrutiny, we reduce the risk of bias still further. Can the particular risk we describe here be reduced to zero? We think not. Replication remains an important safeguard to the scientific endeavour. We now turn our attention to this further safeguard.
Leprosy ulcers are far from the only type of ulcer to which the regenerative medicine solution proposed here is relevant. Diabetic ulcers, in particular, are similar to leprosy ulcers in that loss of neural sensation plays a large part in both. We have argued elsewhere that much can be learned by comparing the results of the same treatment across different disease classes. In due course we hope to collaborate with those who care for other types of skin ulcer so that we can compare and contrast and also to advance methodologically. Together we will seek the optimal method to limit expense and disruption of workflow while minimising outcome bias from reactive measurements.
|
|
|
The CLAHRC WM Director was introduced to Bernard Mandeville's Fable of the Bees by Toby Lewis (CEO of Sandwell & West Birmingham Hospitals NHS Trust) - which famous British economist of the same century was heavily influenced by Mandeville?
Email CLAHRC WM your answer.
|
|
|
Answer to our previous quiz: In economics Kuznet's Curve graphs the hypothesises that as an economy develops, market forces first increase and then decrease economic inequality. The hypothesis was first advanced by economist Simon Kuznet in the 1950-60s.
Congratulations to Hosni Khairy Salem and Alan B Cohen who were first to answer correctly.
|
|
|
Answer to Celia Brown's statistical sprout question: You would need to eat four "chocolates" for a 50% chance of there being at least one sprout. After you’ve taken one and it’s a chocolate the probability the second is a chocolate is then 82/99. Taking four gives a 53% chance of at least one sprout. (p.s. they were awful!)
Congratulations to Jamie Rylance who was first to answer correctly.
|
|
|
Barriers and Facilitators to Self-care of Leprosy in the Community –
Report on a Stakeholder Consultation in Kathmandu, Nepal
The problem
Ulceration and deformity of the extremities, particularly the feet, are important complications of leprosy (known as Hansen’s disease in America). The pathophysiology of leprosy ulcers are similar to those of ulcers in diabetes mellitus – in both cases nerve damage leads to loss of sensation, which in turn leads to repetitive injury and ultimately ulceration. In addition, leprosy causes deformities, which increase the risk of repeated trauma and hence ulceration. Leprosy is a disease that affects the poorest of the poor; frequently those living in remote areas. The disease is highly stigmatising in the communities among whom it occurs leading to late presentation at healthcare facilities and hence a high incidence of ulceration among people who have contracted the disease. Once a person has had one ulcer, repeated ulceration is common, affecting at least 30% of patients.[1]
NIHR CLAHRC WM is working with The Leprosy Mission to develop interventions to prevent ulceration among high risk leprosy patients – especially those who have had previous ulcers. To this effect, we participated in a stakeholder meeting organised by colleagues Drs Deanna Hagge and Indra Napit at the Anandaban Hospital in Kathmandu, Nepal on 14 December 2018.

©Paramjit Gill, 2018. Photo taken with permission of participants.
Stakeholders included leprosy-affected people, ulcer patients, administrative and clinical staff, representatives working on behalf of leprosy affected people, and two government officials. Stakeholders were asked to speak not only about barriers to prevention of ulcers but also possible means to overcome these barriers. All voices were heard and the meeting lasted for about two-hours.
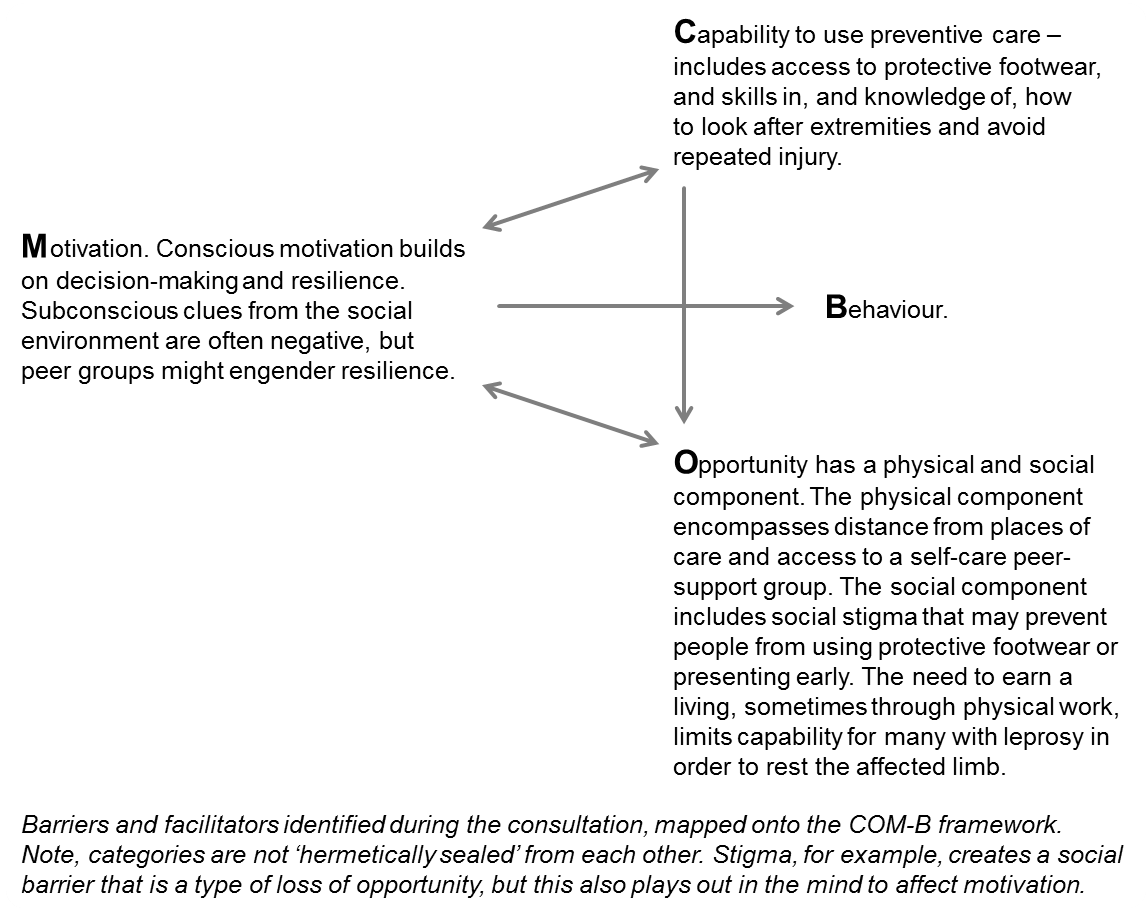
First, we report themes relating to barriers to prevention that emerged during the stakeholder meeting. Second, we arrange them according to the well-known COM-B model [2] encompassing Capability, Opportunity and Motivation as factors affecting Behaviour. Finally, we consider what may be done to overcome the barriers.
Themes
The following themes emerged during the consultation:
- Poverty. All were agreed that the need to work to provide the essentials of life increased the risk of placing pressure on vulnerable foot surfaces and of repeated trauma. Pressure to provide for self and family also increased the risk of late presentation of ulcers or their prodromal signs (so-called ‘hotspots’). One stakeholder commented “If a person cannot work for three months due to wound healing and not putting pressure on the ulcer then how do they live?”
- There was almost unanimous agreement that stigma was a problem, as it led to ‘denial’ (and hence late presentation) and failure to practice self-care and wear protective footwear, which might mark the wearer as a leprosy victim. The view was expressed that stigma reaches its highest intensity in remote rural locations – “some family members don’t know the person has leprosy so question self-care habits such as soaking the hands and feet…in rural areas patients need to hide the wounds and clean them in the night time so nobody sees.”
- Poor information provision. Arguments regarding this barrier were more nuanced. While acknowledging that communication, especially communication pending discharge, was seldom perfect, there was also a feeling that staff tried hard and made a reasonable fist of communicating the essentials of preventative self-care. One stakeholder commented that “leprosy workers are not successful in convincing patients that their body is their responsibility and they have to look after it”. However, convincing patients can be hard, as many people afflicted with leprosy have poor functional literacy. Bridging the gulf in cultural assumptions between care givers and service users may be difficult in a single hospital stay – a point we pursue below.
Analysis according to the ‘trans-theoretical’, COM-B model
We have arranged the above themes using the COM-B model in the Figure. This figure is used to inform the design of interventions that address multiple barriers to healthy behaviours.
 (With thanks to Dr Laura Kudrna for her advice on the Figure).
Designing acceptable interventions
Principles not prescriptions
Interventions to improve care are like guidelines or recipes, not prescriptions. They should not be applied in a one size fits all manner – local implementers should always adapt to context [3] – an intervention as promulgated is not identical to the intervention implemented.[4] Thus, an intervention description at the international level must leave plenty of scope for adaptation of principles to local circumstances that vary within and between countries. For example, peer groups may be more feasible in high than in low burden settings while the development of local health services may determine the extent to which ‘horizontal’ integration between specialist leprosy and general services is possible.
Capability issues
Starting with Capability, there was a feeling that this was not where the main problem lay; patients generally left hospital with the equipment and knowledge that they needed to prepare for life in the community. Our stakeholders said that patients had access to protective footwear (although innovations, such as three dimensional printing to adapt footwear to particular types of defect, would be welcome). Likewise, as stated above, gains to be achieved by an ‘enhanced discharge’ process might be limited. This is for three reasons. First, patients usually receive rather thorough counselling in how to care for themselves during their hospital stay. Second, they usually know the measures to take. Third, understanding is seldom sufficient to bring about behaviour change – school girls who become pregnant are seldom unaware of contraception, for example. In conclusion, a hospital based intervention might not be the most propitious use of scarce resources. This, of course, does not preclude ongoing facility based research to improve treatment and protective methods, nor does it preclude facility outreach activities as we now discuss.
Enhancing ‘Opportunity’
The main barrier identified at the stakeholder meeting seemed to lie in the area of opportunity. Two important principles were established in the meeting. First, since ulcer prevention is an ongoing process its centre of gravity must be located where people live, that is, in the community. Second, peer-supported self-care is a model of established success in leprosy [5,6] (as it has been in diabetes).[7] Two corollaries flow from these considerations. First, where peer support has not been established, this deficiency should be corrected with support from facility based leprosy services. This may take different forms in high burden areas, where groups of people can come together, compared to low burden settings. This suggests that m-health, especially m-consulting, would be particularly useful in low burden settings. Second, where peer support exists (in the form of self-care groups) it should be strengthened, again with support from local facilities who can provide know-how, materials and, we think, inspiration/leadership for ongoing strengthening of locality based support groups. Such support, it was argued, not only provides technical know-how, but importantly, psychological support, to foster resilience and mitigate the pernicious effects of stigma. Telecommunication, when available, will have an important role in coordinating and supporting community self-care. We heard stories of people having to travel for three days to reach a facility; of having to find their way back to remote rural locations with recently healed ulcers on deformed feet and having to complete their journeys on foot. There is a prima facie case that providing mobile telephones will be cost-effective (save in locations so remote they fall outside mobile phone coverage). There was considerable support in the stakeholder meeting for personalised care plans. While accepting the need to individualise, an individual’s needs are not stable. Thus, while specific plans should be made at discharge, it is in the community that adaptations must be made according to changing clinical circumstances, work requirements and personal preferences. In all of the above initiatives, the specialist leprosy services should act as a source of information and psychological/emotional support. Especially in low burden areas, they can act like a poisons facility poisons reference service, providing know how to patients and care providers as and when necessary.
Motivation
As per the legend to our figure, we think that promoting opportunity and motivation go hand in hand in the case of community and outreach services for patients with leprosy who are at risk of ulcers as a result of local anaesthesia and limb deformities. Stigma aggravates the practical and psychological effects of the disease and includes a loss of self-worth and ‘self-stigma’.[8] People with leprosy often have something akin to a ‘crushed spirit’ or ‘chronic depression’ depending on the label one wants to use. Peer supported, facility enabled, self-care may improve motivation. Moreover, emotional support may enable people who have the stigmata left over from active infection to become ambassadors for the condition and help reduce social stigma.
Discussion
It is not enough to say that people suffering the stigma of leprosy should integrate with their communities rather than live in institutions or ‘colonies’, without taking steps to enable them to live in those communities. Such steps are of two types:
- Community level action in supporting /facilitating communities to replace stigma by embracing people with leprosy and actively supporting them.
- Individual support for people with leprosy who are likely to encounter stigma, but who need to prevail in the face of discrimination.
Interventions need to be achievable at low unit cost. So the plan is to design an intervention for propagation across many health systems and to evaluate how it is assimilated locally and what effects it has, within and across multiple contexts. The intervention we propose will involve facility outreach to educate people and ‘teach the teachers’ in communities with the aim of enhancing self-care. There are other actions that might be taken to support people with leprosy (and for that matter other people with disabilities) in the community. One set of measures are those that may alleviate the grinding poverty that many people with leprosy suffer, for instance by providing small loans, non-conditional cash transfers and enterprise coaching. Such interventions, targeting the poorest of the poor have been evaluated and some have proven effective.[9] They may be applicable to people who bear the effects of leprosy and we would be keen to join in the evaluation of such interventions. Information technology would seem to have a large role, as stated above. Diplomatic overtures to opinion formers, such as community leaders, may reduce stigma, especially if people who suffer from ulcers are themselves empowered to advocate on behalf of fellow sufferers. It may be the case that improving care for leprosy sufferers will have spill-over effects on other people with ulcer conditions or physical disabilities. The CLAHRC WM Director would like to thank Drs Indra Napit and Deanna Hagge for organising an excellent meeting, and the attendees for giving their time and sharing their experiences.
-- Prof Richard Lilford, Dr Indra Napit and Ms Jo Sartori
Leave a comment
References
|
|
|
Director's Choice - From the Journals
Demand-Led Research
There is a strange dissonance in the world of health service intervention and research. If a researcher intervenes, then it is necessary to follow a most rigorous pathway of ethics approval and, increasingly, study registration – at least in a prospective study. Read the Ottawa declaration on the ethics of cluster studies [1] or try to register a study on clinicaltrials.gov. As investigator you will need to justify the intervention. All this implies that the investigator is the one in charge of the intervention to be evaluated. How has this poppycock been allowed to persist for so long in a world where improvement projects are endorsed, co-intervention is recited like a catechism, and evidence-based management / service delivery is extolled. While researchers jump through countless hoops, service innovation is all around us – turn up at any board meeting and you will soon realise that evaluated interventions are not just the exception; they are the extreme exception – the tiny tip of a huge iceberg.
This extreme dichotomy makes little sense – if we want to get anywhere then us researchers must tuck in behind and evaluate a higher proportion of the service innovations. And public advisors should raise their sights and worry about the 99.9% of service interventions that are not evaluated. Of course, I am not arguing that all the myriad service evaluations should be evaluated, just a greater proportion – those that are likely to have the greatest financial costs for example, or that may introduce new hazards, or that are more novel. Above all, those which the service managers who control the purse strings are minded to evaluate should be considered.
As a CLAHRC director I have tried to work closely with service managers to meet their needs for evaluation of interventions they have developed - examples will follow over the course of this year.
-- Richard Lilford, CLAHRC WM Director
Leave a comment
Reference
Process of Diagnosis
I have had a long-stranding fascination with diagnosis. The medical school I attended at the University of Witwatersrand was arguably the world’s premier institution for medical training at the time. My teachers, such as Thomas Bothwell, Leo Schamroth and ‘Sonny’ du Plessis, were the foremost practitioners and teachers of their time. They were famed for their diagnostic prowess.
In those days, diagnosis worked in a careful, bottom-up way – like a detective investigating a case. Careful collection of clinical features, logical analysis of the findings, a list of possibilities, and judicious use of targeted testing.
Now diagnosis has become more of a two-way street. Take a recent paper in the New England Journal of Medicine [1] describing an organisation in Boston (where else?) called the Undiagnosed Diseases Network (UDN) – a sort of option of last resort for the patient who emerges unclassified despite a ‘thicket of investigations’. Here the diagnostic process is more like speed-dating – we look for a ‘match’. In the case of diagnosis, a computer matches phenotype to genotype – no hypothesis formation and rational deduction needed. The UDN centre offers to match clinical features and standard lab tests to genotype. The study by Splinter and colleagues reports on 1,519 patients referred over a 20 month period, of whom 382 received the full diagnostic work up. Forty percent of these 385 had, as you would have intuited, a neurological condition. Just over a third (132 of the 382) received a diagnosis. Thirty-five of these diagnoses were previously undescribed syndromes and the diagnosis was made by gene sequencing by the UDN in 98 of the 132 patients. Genetic counselling was indicated in 36% of cases and a change of therapy in 21%.
This is a most fascinating paper and a foretaste of things to come – it can’t be long before patients match their features to databases and discover yet more new diseases they can name after themselves.
-- Richard Lilford, CLAHRC WM Director
Leave a comment
Reference
Risk of Death or Readmission over Christmas Period
I thank Prof Kamlesh Khunti for drawing my attention to this article.[1] It uses a Canadian database of hospital use to compare the outcomes for patients admitted over the Christmas period with those admitted over two control periods of one month on either side of the holiday. The study finds that there were less subsequent outpatient attendances, but more deaths or readmissions, for patients discharged over the Christmas period when compared to those admitted over the control periods.
What to make of such a study? Is it really the case that the reduction in outpatient supervision is the cause of the deaths or readmissions? Certainly, if one looked only at deaths, the difference is minute, although statistically significant after adjustment for confounders. The trouble is that small magnitudes of effects can be the result of small biases, which are impossible to detect statistically.
All the same, this is an interesting study and it might be worthwhile to try and replicate it on an English data set..
-- Richard Lilford, CLAHRC WM Director
Leave a comment
Reference
Ringing Endorsement for Bayesian Statistics from
World’s Top Scientific Journal
I have long railed against the use of p-Values and frequentist confidence limits in medical decision making. Stephen Goodman, a hero of mine, takes up this theme in a recent issue of Nature.[1] He attacks the persisting misconception that the p-Value is a measure of the probability that the null hypothesis is true. This stubborn misconception led the American Statistical Association to issue a public statement in 2016 discouraging ‘bright line’ p-Value thresholds.[2]
The time is coming when statisticians, who all understand that the p-Value is not a measure of the probability of some hypothesis, apply the knowledge in their work with applied researchers. Sticking to p-Values and confidence limits puts statisticians on top when they should, instead, be on tap.
-- Richard Lilford, CLAHRC WM Director
Leave a comment
References
Return to top
|
|
|
|
Re: A Bigger Risk Than Climate Change?
Thank you for your thought-provoking article highlighting the non-negligible risk of a nuclear war given the devastation it could cause. Apart from the scale of immediate life loss and prolonged burden of ill health such a warfare could bring about as you demonstrated in your calculation, perhaps the issue deserves a little more attention also because we know relatively little about how to robustly prevent such an event from happening (although colleagues in political sciences might disagree!) - compared with the ever growing knowledge base that we now possess concerning the causes and mechanisms of climate change and human diseases, based on which we can draw up clear action plans. It appears to be a high time for behaviour sciences and psychology to solve health care problems in health services research. I wonder if you are foreseeing a similar trend at macro level, for political sciences to address ultimate welfare issues of human being.
-- Yen-Fu Chen, Associate Professor
Another potentially catastrophic event that has a high likelihood of occurring is a large Solar flare – a repeat of the Carrington event of 1859. In the world of the mid 19th century a large solar flare impacting on the world had minimal adverse effects other then blowing out some telegraph wires. Should the same flare strike today many, if not most, communication satellites would be destroyed and, if there was no preparation then the electrical grid would fail with destruction of a large proportion of electrical transformers, which means that the grid may be down for weeks or months across large parts of the world. Losing electrical power for weeks or months would have devastating effects on economic activity and lead to a large loss of life. Relatively simple steps can be taken to mitigate the most serious effects, one of which is to boost satellite detection of the flare, which would give us many hours if not days notice of a coronal mass ejection, which would allow us to safely shut down the electrical grid for a few hours whilst the storm passes. A similar flare to the Carrington event missed the earth by a few days in 2012 – so these events are quite common and will inevitably strike the earth.
-- D Torgerson
I recently saw this image of what to do in the event of a nuclear strike at Christmas and thought of your blog!
-- Oyinlola Oyebode, Associate Professor
Author's Response: Thanks for the comments - I hope that the Cabinet Office has clocked solar flares on their risk of population hazard.
-- Richard Lilford, CLAHRC WM Director
Re: Vitamin D and Schizophrenia
It is amazing how much time and money were spent during last 20 years for the studies of the possible treatment|prevention uses oа the vitamin D. And almost all failed. Was it just fashion? Or this subject was fundable?
-- Ivo Vlaev, Professor of Behavioural Science
Return to top
|
|
|
|
Jones E, Taylor B, Rudge G, MacArthur C, Jyothish D, Simkiss D, Cummins C. Hospitalisation after birth of infants: cross sectional analysis of potentially avoidable admissions across England using hospital episode statistics. BMC Pediatr. 2018; 18(1): 390.
Kuo C-F, Chou I-J, Rees F, Grainge MJ, Lanyon P, Davenport G, Mallen CD, Chung T-T, Chen J-S, Zhang W, Doherty M. Temporal relationships between systemic lupus erythematosus and comorbidities. Rheumatol. 2018.
Taylor C, Joolay Y, Buckle A, Lilford R. Prioritising allocation of donor human breast milk amongst very low birthweight infants in middle-income countries. Mat Child Nutr. 2018; 14(s6).
Return to top
|
|
|
|
|
|
|
|
|